马дёҠжіЁеҶҢпјҢз»“дәӨжӣҙеӨҡеҘҪеҸӢпјҢдә«з”ЁжӣҙеӨҡеҠҹиғҪпјҢи®©дҪ иҪ»жқҫзҺ©иҪ¬зӨҫеҢәгҖӮ
жӮЁйңҖиҰҒ зҷ»еҪ• жүҚеҸҜд»ҘдёӢиҪҪжҲ–жҹҘзңӢпјҢжІЎжңүиҙҰеҸ·пјҹз«ӢеҚіжіЁеҶҢ

x
жң¬её–жңҖеҗҺз”ұ иҖҒ马 дәҺ 2014-11-24 16:44 зј–иҫ‘
) I, ~0 z: g/ P- B: m2 r: g; C2 C: u6 s. j0 \3 k. e n
жҒ¶жҖ§иӮҝзҳӨжӮЈиҖ…йЈҹж¬ІдёҚдҪідё»иҰҒдёҺжҒ¶жҖ§иӮҝзҳӨзҡ„з”ҹй•ҝгҖҒиӮҝзҳӨз ҙеқҸиҝҮзЁӢдёӯжҜ’зҙ зҡ„йҮҠж”ҫгҖҒжүӢжңҜгҖҒж”ҫеҢ–з–—е’Ңйқ¶еҗ‘иҚҜзҡ„еүҜдҪңз”ЁеҸҠеҝғзҗҶеӣ зҙ зӯүжңүе…ігҖӮ6 G8 p, h y h$ M) j( \
жҒ¶жҖ§иӮҝзҳӨз—…дәәиғҪйҮҸгҖҒзўіж°ҙеҢ–еҗҲзү©гҖҒи„ӮиӮӘеҸҠиӣӢзҷҪиҙЁд»Ји°ўеқҮжңүеҫҲеӨ§зЁӢеәҰзҡ„ж”№еҸҳгҖӮиғҪйҮҸж¶ҲиҖ—еўһеҠ е’ҢдҪҺж•ҲзҺҮзҡ„иғҪйҮҸеҲ©з”Ёеёёиў«и®ӨдёәжҳҜиҚ·зҳӨжңәдҪ“иҗҘе…»дёҚиүҜзҡ„еҺҹеӣ гҖӮжңәдҪ“зҡ„еҹәзЎҖд»Ји°ўзҺҮдёҺз–ҫз—…иҝӣзЁӢеҸҠиҗҘе…»зү©иҙЁж‘„е…ҘжҲҗеҸҚжҜ”дҫӢгҖӮжҒ¶жҖ§иӮҝзҳӨз—…дәәзҡ„д№ій…ёеҫӘзҺҜжҙ»жҖ§еўһеҠ пјҢеңЁиҝҷдёҖж— з”Ёзҡ„еҫӘзҺҜдёӯпјҢи‘Ўиҗ„зі–иў«иҪ¬еҢ–дёәд№ій…ёпјҢ继иҖҢеҸҲеңЁиӮқз»ҶиғһеҶ…иҪ¬еҢ–дёәи‘Ўиҗ„зі–пјҢиҝҷз§ҚдҪҺж•Ҳзҡ„еҫӘзҺҜеҗҢж—¶иҝҳжҳҜдёҖдёӘиҖ—иғҪиҝҮзЁӢпјҢз—…дәәзҡ„д№ій…ёеҫӘзҺҜжҙ»жҖ§и¶Ҡй«ҳпјҢиғҪйҮҸж¶ҲиҖ—и¶ҠеӨ§пјҢдҪ“йҮҚеҮҸе°‘д№ҹи¶ҠжҳҺжҳҫгҖӮжҒ¶жҖ§иӮҝзҳӨжңәдҪ“еҜ№иғ°еІӣзҙ зҡ„ж•Ҹж„ҹжҖ§еҫҖеҫҖеҸ—жҚҹпјҢи‘Ўиҗ„зі–иҖҗеҸ—жҖ§дёӢйҷҚпјҢз—…дәәиӮҢиӮүе’ҢиӮқи„ҸдёӯеҶ…жәҗжҖ§зі–еҺҹиҙ®еӨҮиҫғе°‘пјҢзЁҚжңүйҘҘйҘҝеҚіеҸҜиҖ—е°ҪпјҢиҖҢзҘһз»Ҹз»Ҷиғһе’Ңзәўз»ҶиғһеҜ№и‘Ўиҗ„зі–зҡ„еҲ©з”Ёд»ҚеңЁиҝӣиЎҢпјҢжңәдҪ“еҲҶи§ЈиӣӢзҷҪиҙЁиҝӣиЎҢзі–ејӮз”ҹгҖӮеңЁйқһзҷҢз—Үз—…дәәгҖҒиӮҢиӮүиӣӢзҷҪиҙЁеҲҶи§ЈйҖҗжёҗз”ұи„ӮиӮӘд»Ји°ўжүҖд»ЈжӣҝпјҢи„ӮиӮӘй…ёиҪ¬еҢ–дёәй…®дҪ“з»ҷжңәдҪ“дҫӣиғҪпјҢд»ҺиҖҢиҠӮзңҒиӮҢиӮүиӣӢзҷҪгҖӮиҖҢеңЁзҷҢз—Үз—…дәәпјҢжңәдҪ“дё§еӨұдәҶдёәеә”жҝҖзҠ¶жҖҒдёӢжүҖи®ҫзҪ®зҡ„дҝқеӯҳдҪ“иӣӢзҷҪзҡ„жӯЈеёёжңәеҲ¶пјҢз»“жһңи‘Ўиҗ„зі–дә§з”ҹеўһеҠ пјҢеҗҢж—¶иӣӢзҷҪиҙЁеҲҶи§Јд№ҹеўһеҠ пјҢиӮҢиӮүиӣӢзҷҪиҙЁеҗҲжҲҗеҮҸе°‘пјҢжңәдҪ“ж°®дёўеӨұпјҢиЎҖжё…ж°Ёеҹәй…ёи°ұејӮеёёгҖӮ30%~100%иҝӣеұ•жңҹжҒ¶жҖ§иӮҝзҳӨз—…дәәе‘Ҳиҙҹж°®е№іиЎЎгҖӮ; I# o& P' `9 Z1 W0 C9 z
дёҖгҖҒж”№еҸҳйҘ®йЈҹд№ жғҜ
; }0 S1 C0 K @& M$ q1гҖҒе°‘йЈҹеӨҡйӨҗпјҢжҸҗдҫӣй«ҳиғҪйҮҸгҖҒй«ҳиӣӢзҷҪиҙЁйҘ®йЈҹжҲ–иҗҘе…»иЎҘе……е“ҒгҖӮ7 }$ C$ t5 i/ t: g! o6 Y; V* J% J
2гҖҒжӣҙжҚўйЈҹи°ұпјҢе°қиҜ•з”Ёеҗ„з§Қжё©е’Ңзҡ„и°ғе‘іж–ҷпјҢз»ҸеёёеҸҳеҢ–зғ№йҘӘж–№ејҸдёҺеҪўжҖҒпјҢеўһејәиүІйҰҷе‘ігҖӮ
; q/ V& b& I; j# V1 w5 q1 y/ U4 x+ n3гҖҒйӨҗеүҚеҒҡйҖӮйҮҸзҡ„иҝҗеҠЁпјҲжҜ”еҰӮж•ЈжӯҘпјүжҲ–йЈҹз”ЁејҖиғғйЈҹзү©гҖӮ1 T# q! L Q! I: L5 c
4гҖҒиҝӣйӨҗж—¶еә”дҝқжҢҒж„үеҝ«зҡ„еҝғжғ…пјҢеҸҜд»Ҙи§ӮзңӢе–ңж¬ўзҡ„з”өи§ҶиҠӮзӣ®жҲ–иҖ…ж’ӯж”ҫиҪ»йҹід№җгҖӮ
# a. H! \/ x* e T$ o' V5гҖҒз”ЁйӨҗж—¶е…ҲйЈҹз”ЁеӣәдҪ“йЈҹзү©пјҢеҶҚйҘ®з”Ёж¶ІдҪ“жұӨжұҒжҲ–йҘ®ж–ҷгҖӮ
) H, o& i6 |8 ^3 `6гҖҒиӢҘж„ҹи§үз–ІеҠіпјҢеә”дј‘жҒҜзүҮеҲ»пјҢеҫ…дҪ“еҠӣжҒўеӨҚеҗҺеҶҚиҝӣйЈҹгҖӮе°ҪйҮҸе°‘ж‘„е…ҘжІ№и…»йЈҹзү©гҖӮ" x. X5 L# x* P1 L% B7 u$ R$ V
7гҖҒжҜҸеӨ©иЎҘе……йҖӮйҮҸзҡ„з»ҙз”ҹзҙ гҖҒзҹҝзү©иҙЁгҖҒж°ҙеҲҶгҖӮ
/ s& L( b. e7 x8гҖҒдҪҝз”ЁеӨ§зҡ„зў—зўҹзӣӣйЈҹзү©пјҢжҳҫеҫ—д»ҪйҮҸдёҚеӨҡгҖӮ/ J5 D. \& C1 V' | V4 j; v4 |
дәҢгҖҒеёёз”ЁиҚҜзү©# r/ F4 @3 E1 p6 s& q2 j8 L3 H
1гҖҒжҠ—жҒ¶еҝғиҚҜзү©пјҡиғғеӨҚе®ү(metoclopramide)# E4 q& t' l0 \/ F
2гҖҒдҝғиҝӣйЈҹж¬ІиҚҜзү©пјҡ
3 Y K/ f! e wеӣӣзЈЁжұӨеҸЈжңҚж¶І6 L; T" k }0 @6 L
з”Іең°еӯ•й…®пјҲMegestrol acetateпјүпјҡ160mgжҜҸеӨ©пјҢдёҖеӨ©дёҖж¬ЎеҸЈжңҚпјҢ7-28еӨ©гҖӮпјҲз”Іең°еӯ•й…®зҡ„еүӮйҮҸд»Һ160mgжҜҸеӨ©еўһеҠ еҲ°320~480mgжҜҸеӨ©пјҢдҪ“йҮҚеўһеҠ жӣҙеӨҡпјҢиҖҢйЈҹж¬Іж”№е–„ж— еҢәеҲ«гҖӮжӣҙй«ҳзҡ„еүӮйҮҸпјҢж— жӣҙеӨҡзҡ„зӣҠеӨ„гҖӮпјү; K" p) o' S: k6 s, ]+ U# ^$ C
ең°еЎһзұіжқҫпјҲdexamethasoneпјүпјҡжҜҸеӨ©2-4mgпјҢдёҖеӨ©еҲҶдәҢж¬ЎеҸЈжңҚгҖӮ
5 ]1 y; |+ f2 w) I/ y8 VеӨ§йә»жҸҗеҸ–зү©пјҡеӣӣж°ўеӨ§йә»й…ҡпјҲDronabinolпјүпјҢеӣӣж°ўеӨ§йә»йҶҮпјҲcannabinoidпјүзӯү
& r7 ~6 }: J8 a6 u8 S q3гҖҒеҠ©ж¶ҲеҢ–иҚҜзү©пјҡеӨҡй…¶зүҮ
% h0 C/ S; N+ o+ B* p+ p" C4гҖҒдҝғиғғиӮ еҠЁеҠӣиҚҜпјҡеҗ—дёҒе•үпјҲеӨҡжҪҳз«Ӣй…®пјү(domperidone)гҖҒиҘҝжІҷжҜ”еҲ©(cisaprideгҖҒprepulsid,жҷ®з‘һеҚҡжҖқ)гҖҒиҺ«жІҷжҜ”еҲ©пјҲMosapride ,иҙқз»ңзәіпјҢеҠ ж–Ҝжё…пјүгҖҒжӣҝеҠ иүІзҪ—(TegaserodпјҢжіҪ马еҸҜ)гҖӮ
' f, W7 o8 K j( E& K+ L `5гҖҒеҫ®з”ҹжҖҒеҲ¶еүӮпјҡеҹ№иҸІеә·(Bifico, еҸҢжӯ§дёүиҒ”жҙ»иҸҢиғ¶еӣҠ)+ [' T d" z. A$ D2 f6 G
6гҖҒжҠ—жҠ‘йғҒиҚҜпјҡзұіе°”еЎ”жүҺе№іпјҲmirtazapineпјүгҖҒзҷҫеҝ§и§ЈпјҲProzacпјү
$ u ^4 a6 B' L D6 J2 d! xдёүгҖҒжҺЁиҚҗзҡ„дҝқеҒҘе“Ғ7 `5 T% {6 G/ Z
1гҖҒйӣҖе·ўзҡ„йҖҹж„Ҳзҙ гҖҒйӣ…еҹ№зҡ„дҝқеә·йҖҹе’Ңе®үзҙ
" v c5 u# @0 ?+ y. f7 J! d+ i2гҖҒжө·еҸӮ. n$ j' I) U9 i( t4 u R$ K
3гҖҒд№ій“ҒиӣӢзҷҪ) j P6 R6 O% e. y7 _
еӣӣгҖҒиҗҘе…»ж”ҜжҢҒдёҺиӮҝзҳӨз”ҹй•ҝзҡ„е…ізі»
' _- f6 h. b' F7 W kеҜ№иӮҝзҳӨз—…дәәиҝӣиЎҢиҗҘе…»ж”ҜжҢҒж—¶пјҢдәә们еҸҜиғҪжӢ…еҝғиҗҘе…»ж”ҜжҢҒеҸҜиғҪдјҡдҪҝиӮҝзҳӨеҸ—зӣҠгҖӮеҠЁзү©е®һйӘҢиЎЁжҳҺпјҢиҗҘе…»ж”ҜжҢҒеңЁж”№е–„иҚ·зҳӨе®ҝдё»иҗҘе…»зҠ¶еҶөзҡ„еҗҢж—¶пјҢеҜ№иӮҝзҳӨз»ҶиғһеҠЁеҠӣеӯҰд№ҹдә§з”ҹеҪұе“ҚпјҢеҸҜеҜјиҮҙиӮҝзҳӨз»„з»ҮиӣӢзҷҪеҗҲжҲҗеўһеҠ пјҢиӮҝзҳӨз»ҶиғһDNAгҖҒRNAеҗ«йҮҸеўһй«ҳпјҢиҮҙиӮҝзҳӨз”ҹй•ҝйҖҹеәҰеҠ еҝ«гҖӮе®һйҷ…дёҠпјҢдәәдҪ“иӮҝзҳӨдёҺеҠЁзү©е®һйӘҢзҡ„иӮҝзҳӨжңүиҫғеӨ§зҡ„е·®еҲ«гҖӮеҠЁзү©з§»жӨҚжҖ§иӮҝзҳӨеҖҚеўһж—¶й—ҙзҹӯпјҢеўһй•ҝиҝ…йҖҹпјҢжӯ»дәЎеҝ«пјҢиӮҝзҳӨеҚ жҖ»дҪ“зҡ„30%д»ҘдёҠпјҢиҝҷдәӣзү№зӮ№еҸҜиғҪжҳҜе®һйӘҢжҖ§иӮҝзҳӨеҜ№иҗҘе…»зјәд№Ҹиҫғдёәж•Ҹж„ҹзҡ„еҺҹеӣ гҖӮиҖҢдәәдҪ“иӮҝзҳӨеўһй•ҝйҖҹеәҰзӣёеҜ№иҫғж…ўпјҢдёҖиҲ¬дёҚи¶…иҝҮжҖ»дҪ“зҡ„5%пјҢе®һдҪ“зҳӨзҡ„е№іеқҮеҖҚеўһж—¶й—ҙдёә100еӨ©гҖӮеӣ жӯӨпјҢеҝ…иҰҒзҡ„иҗҘе…»ж”ҜжҢҒдёҚеҸҜиғҪеңЁзҹӯжңҹеҶ…еҜ№иӮҝзҳӨзҡ„еўһй•ҝдә§з”ҹеҫҲеӨ§зҡ„еҪұе“ҚгҖӮ; w" K' ]! s `
ж №жҚ®еӨ§йҮҸзҡ„ж°Ёеҹәй…ёдёҺиӮҝзҳӨз”ҹй•ҝзҡ„з ”з©¶еҸ‘зҺ°пјҢе№іиЎЎж°Ёеҹәй…ёиғҪдҝғдҪҝиӮҝзҳӨз»ҶиғһиӣӢзҷҪиҙЁеҗҲжҲҗеҠ йҖҹпјҢSжңҹз»ҶиғһзҷҫеҲҶжҜ”еўһеҠ пјҢжңүдёқеҲҶиЈӮжҙ»жҖ§еўһејәпјҢдҪҝиӮҝзҳӨдҪ“з§Ҝеўһй•ҝиҝ…йҖҹпјҢиҖҢй«ҳжө“еәҰзІҫж°Ёй…ёгҖҒиӣӢж°Ёй…ёзјәд№Ҹзҡ„дёҚе№іиЎЎж°Ёеҹәй…ёеҸҜдҪҝиӮҝзҳӨз»Ҷиғһзҡ„еўһж®–еҸ—еҲ°жҠ‘еҲ¶гҖӮ
6 R- n$ o* H4 y/ U& z$ gж №жҚ®жҹҗдәӣж°Ёеҹәй…ёеңЁиӮҝзҳӨз”ҹй•ҝдёӯзҡ„зү№ж®ҠдҪңз”Ёе’ҢиӮҝзҳӨз»Ҷиғһзҡ„д»Ји°ўзү№зӮ№пјҢдәәдёәең°ж”№еҸҳж°Ёеҹәй…ёзҡ„常规еүӮйҮҸпјҢеҲ¶жҲҗжҹҗз§Қж°Ёеҹәй…ёиҝҮйҮҸжҲ–еҮҸе°‘д№ғиҮізјәеӨұзҡ„ж°Ёеҹәй…ёеӨұиЎЎж¶ІдёәиӮҝзҳӨз—…дәәиҝӣиЎҢиҗҘе…»ж”ҜжҢҒпјҢд»ҘиҫҫеҲ°жҠ‘еҲ¶иӮҝзҳӨз”ҹй•ҝеҸҲиғҪж”№е–„з—…дәәиҗҘе…»зҠ¶еҶөзҡ„зӣ®зҡ„гҖӮзӣ®еүҚз ”з©¶иҫғеӨҡзҡ„жңүеҺ»LпјҚзј¬ж°Ёй…ёеӨұиЎЎж¶ІгҖҒеҺ»LпјҚиӣӢж°Ёй…ёеӨұиЎЎж¶ІгҖҒеҺ»LпјҚиӢҜдёҷж°Ёй…ё/й…Әж°Ёй…ёеӨұиЎЎж¶ІпјҢд»ҘеҸҠLпјҚзІҫж°Ёй…ёеўһйҮҸеӨұиЎЎж¶ІзӯүгҖӮ3 A M. t2 I6 t/ C. n, ]
иӣӢзҷҪиҙЁзҡ„ж‘„е…ҘиҝҮдҪҺжҲ–иҝҮй«ҳеқҮдјҡдҝғиҝӣиӮҝзҳӨзҡ„з”ҹй•ҝгҖӮиӣӢзҷҪиҙЁзҡ„ж‘„е…ҘйҮҸеә”йҖӮйҮҸгҖӮдёҖиҲ¬жҲҗе№ҙдәәиӣӢзҷҪиҙЁеҚ жҖ»зғӯиғҪзҡ„12пј…вҖ”15пј…пјҢжҜҸеӨ©ж‘„е…Ҙ70вҖ”80gдёәе®ңгҖӮ
* p3 X# m+ H5 P- y ?, y: y, gжҒ¶жҖ§иӮҝзҳӨжӮЈиҖ…иЎҖжё…й”ҢйҷҚдҪҺгҖҒй“ңеҚҮй«ҳпјҢй“ң/й”ҢжҜ”еҖјеҚҮй«ҳеҸҜи§ҒдәҺд»»дҪ•йғЁдҪҚзҡ„жҒ¶жҖ§иӮҝзҳӨпјҢжҳҜжҒ¶жҖ§иӮҝзҳӨзҡ„е…ұеҗҢзү№еҫҒгҖӮдёҖиҲ¬и®ӨдёәпјҢиӮҝзҳӨжөёж¶ҰиҢғеӣҙи¶Ҡе№ҝгҖҒз—…жңҹи¶ҠжҷҡпјҢиЎҖжё…й“ңи¶Ҡй«ҳгҖҒй”Ңи¶ҠдҪҺгҖӮиЎҖжё…й“ңи¶Ҡй«ҳпјҢжӮЈиҖ…зҡ„з”ҹеӯҳжңҹи¶ҠзҹӯпјҢйў„еҗҺи¶Ҡе·®гҖӮ, b; }2 y1 E$ t6 g! w6 y. d
2 E3 v4 {5 c) U5 o1 ~( o1 {! b=====================5 g9 c6 g W9 p* }( U; k' @) b
Enobosarm improves muscle wasting experienced by patients with NSCLC., t. k, Y$ F5 ?* w6 n
http://ecancer.org/news/4073-emc ... ents-with-nsclc.php- y6 | h. h/ X, }+ K
A randomised, double-blind, placebo controlled phase IIB trial shows that treatment with enobosarm, a non-steroidal selective androgen receptor modulator, significantly improved one measure of physical function and increased lean muscle mass in cancer patients overall and specifically in a cohort of patients with non-small cell lung cancer (NSCLC).' n, h6 k% z7 K
1 [ c1 u1 o( f% E( }: i' p* b
Dr Christopher Croot of the Department of Hematology and Oncology, North Mississippi Hematology and Oncology Associates, Ltd. Tupelo, USA is a first author of the study which findings were complied in a poster-discussion and presented at the European Multidisciplinary Conference in Thoracic Oncology (EMCTO).; t4 E7 K8 E% \+ b+ A( P) e
% N1 }0 H! S. g: g2 LMuscle wasting is a hallmark of cachexia which is caused by byproducts produced by some forms of cancer or by the body's reaction to it.
6 ^4 x# N0 ^% O: M; ^
T2 \/ H! [2 B U- q6 F6 cMuscle wasting typically affects skeletal muscles, negatively affecting physical function.8 t" S2 N0 y+ y9 }* i5 ^" u, g
7 ^+ H! f% l$ Q$ I0 Q& |9 _5 JIt is estimated that more than 50% of lung cancer patients already demonstrate muscle wasting at diagnosis, which increases to affect more than 80% of patients prior to dying from their disease.2 `: Z) q' r! P4 j |$ U3 M& m
# c7 N% S6 l& e \6 CEnobosarm is non-steroidal selective androgen receptor modulator that is tissue-selective and has anabolic effects in muscle and bone, thus increasing lean body mass.
6 C, z5 T1 {; V6 G7 P/ Z
# n+ Z9 m. W" G& |This randomised, double-blind, placebo controlled study evaluated the effect of enobosarm on lean body mass and physical function in a subset of NSCLC patients.6 g& u7 |" Y9 E- s1 b; K3 W
( v' W; ^3 i! B8 gThe study enrolled males aged 45 years or more and postmenopausal females, who experienced weight loss of 2% or more over the preceding 6 months. The study participants had been diagnosed with NSCLC, colorectal cancer, non-HodgkinвҖҷs lymphoma, chronic lymphocytic leukaemias, or breast cancer. A4 l0 A" @0 `
0 {/ d0 t' D8 p$ m( j* _9 l
The study primary and secondary endpoints were change in lean body mass as determined by dual energy X-ray absorptiometry (DEXA) scan and physical function measured by stair climb power, respectively. Response was defined as either a 10% improvement in stair climb power or no loss in lean body mass.' p# m1 ~1 L6 h' G* {
+ k j& P4 T; o5 J
A total of 159 study participants, including a subset comprised of 61 patients with NSCLC, received enobosarm at doses of 1mg or 3mg or placebo for 16 weeks. At 16 weeks, patients treated with enobosarm achieved statistically significant improvements compared to baseline in stair climb power and lean body mass that were not seen in the patients who received placebo.! P, M& q; v0 \, y0 u
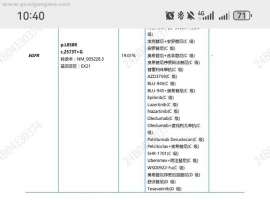
9 i9 {. ~2 ?3 o! D# i3 ?9 yAmong 28 NSCLC patients who were evaluable for stair climb power, 18 enobosarm treated subjects showed an improvement of median 17% over baseline that was statistically significant (p=0.007). Among the 31 NSCLC subjects who were evaluable for lean body mass, the enobosarm cohort of 21 patients showed a median 1.0 kg increase in lean body mass; whereas, a 0.8 kg loss of lean body mass was observed in patients receiving placebo. The responder analysis demonstrated that 78% and 67% of enobosarm treated patients met the criteria defining stair climb power and lean body mass response, respectively.
' i: [; b& y; J! G, ?% R
+ Z( ?& e3 j8 @# t+ z4 l0 m+ REnobosarm was well tolerated and commonly reported adverse events were consistent with adverse events seen with chemotherapy and included fatigue, anaemia, nausea, and diarrhoea.
2 \" @- M3 o6 u. Z5 z" ~1 }' p: n! ]
On Friday April 12, 2013, an independent Data Safety Monitoring Board (DSMB) announced that a per protocol safety review of unblinded safety data supported the two pivotal phase III clinical trials of enobosarm that are ongoing to determine the prevention and treatment of muscle wasting in patients with advanced NSCLC.9 O: G- ~# I X4 [. r4 p. h
1 p x T/ {# E" @! _0 q9 Q1 aDuring the time foreseen for questions and answers, the first author of the study said that two ongoing phase III studies evaluate enobosarm with different type of chemotherapy, one investigate platinum and taxane-based chemotherapy, while the second evaluate platinum and non-taxane regimen. It is important because it is well known that chemotherapy itself can treat symptoms in patients with NSCLC. Each of these phase III studies enrolled 320 patients. The last patient has been enrolled last week. The second point raised during the discussion was that the study authors did not prospectively investigate on the use of glucocorticoids. It would be also important in such studies to test androgen receptor in tumour tissue, however the study presenter said that it has been for a long time speculated on role of testosterone and more lung cancer rates in men than in women, however he doesn't believe the androgen receptor has a major impact on the outcome in NSCLC.
' z5 b/ s* x* Q6 ~+ z |
-
1
жҹҘзңӢе…ЁйғЁиҜ„еҲҶ
-
|


 дёҖзәҝзӣҙжҺҘеҗғдјҸзҫҺжӣҝе°јпјҢеҰӮдҪ•е»¶й•ҝиҖҗиҚҜпјҹ
2024е№ҙ9жңҲзЎ®иҜҠиӮәи…әзҷҢпјҢ4aжңҹпјҢеҹәеӣ жЈҖжөӢз»“жһңеҰӮдёӢеӣҫпјҢзЎ®иҜҠеҗҺеҗ¬еҢ»з”ҹзҡ„зӣҙжҺҘеҗғдёүд»ЈиҚҜдјҸзҫҺдәҶ
дёҖзәҝзӣҙжҺҘеҗғдјҸзҫҺжӣҝе°јпјҢеҰӮдҪ•е»¶й•ҝиҖҗиҚҜпјҹ
2024е№ҙ9жңҲзЎ®иҜҠиӮәи…әзҷҢпјҢ4aжңҹпјҢеҹәеӣ жЈҖжөӢз»“жһңеҰӮдёӢеӣҫпјҢзЎ®иҜҠеҗҺеҗ¬еҢ»з”ҹзҡ„зӣҙжҺҘеҗғдёүд»ЈиҚҜдјҸзҫҺдәҶ
 еҘҘиҘҝжӣҝе°јиҖҗиҚҜеҗҺз»ӯжІ»з–—пјҢеҮәзҺ°и…№ж°ҙ
жІ»з–—з»ҸиҝҮпјҡ
2010зЎ®иҜҠи…әзҷҢ
жІ»з–—ж–№жЎҲпјҡеҸіиӮәдёҠеҸ¶еҲҮйҷӨпјҢ10е№ҙж°‘иҜәе®ҫ2ж¬ЎпјҢйЎәй“Ӯ+зӣ–иҜә2ж¬ЎгҖӮ
еҘҘиҘҝжӣҝе°јиҖҗиҚҜеҗҺз»ӯжІ»з–—пјҢеҮәзҺ°и…№ж°ҙ
жІ»з–—з»ҸиҝҮпјҡ
2010зЎ®иҜҠи…әзҷҢ
жІ»з–—ж–№жЎҲпјҡеҸіиӮәдёҠеҸ¶еҲҮйҷӨпјҢ10е№ҙж°‘иҜәе®ҫ2ж¬ЎпјҢйЎәй“Ӯ+зӣ–иҜә2ж¬ЎгҖӮ
 иҝҷжҳҜиҖҗиҚҜдәҶеҗ—пјҹ
2024е№ҙ8жңҲд»ҪзЎ®иҜҠиӮәи…әзҷҢеӣӣжңҹпјҢејҖе§ӢеҚЎй“Ӯ+еҹ№зҫҺжӣІеЎһ+зү№з‘һжҷ®еҲ©жІ»з–—6ж¬ЎпјҢжңҹй—ҙжҜҸдёӨж¬ЎжІ»з–—еҗҺеӨҚ
иҝҷжҳҜиҖҗиҚҜдәҶеҗ—пјҹ
2024е№ҙ8жңҲд»ҪзЎ®иҜҠиӮәи…әзҷҢеӣӣжңҹпјҢејҖе§ӢеҚЎй“Ӯ+еҹ№зҫҺжӣІеЎһ+зү№з‘һжҷ®еҲ©жІ»з–—6ж¬ЎпјҢжңҹй—ҙжҜҸдёӨж¬ЎжІ»з–—еҗҺеӨҚ
 дёәд»Җд№ҲиӮәзҷҢжӮЈиҖ…йңҖиҰҒMDTпјҹдёүдёӘз–‘йҡҫз—…
ж•ҙзҗҶпјҡ淡然清欢гҖҒеј еёҶгҖҒе№ҙеҺ»еІҒжқҘгҖҒйӣЁиҝҮеӨ©жҷҙе®Ўж ёпјҡеј и•»жў…гҖҒй’ұе“ІгҖҒй№°зүҲеңЁеҪ“дёӢзҡ„иӮҝзҳӨжІ»з–—
дёәд»Җд№ҲиӮәзҷҢжӮЈиҖ…йңҖиҰҒMDTпјҹдёүдёӘз–‘йҡҫз—…
ж•ҙзҗҶпјҡ淡然清欢гҖҒеј еёҶгҖҒе№ҙеҺ»еІҒжқҘгҖҒйӣЁиҝҮеӨ©жҷҙе®Ўж ёпјҡеј и•»жў…гҖҒй’ұе“ІгҖҒй№°зүҲеңЁеҪ“дёӢзҡ„иӮҝзҳӨжІ»з–—
 дёҖеҝғдёҖзӣҠпјҢдёҺзҲұеҗҢи·‘пјҢ第еӣӣеұҠе…¬зӣҠи·‘жҠҘ
дҪңиҖ…пјҡpear
иҰҒиҜҙд»Ҡе№ҙи°ҒжңҖеҮәеңҲпјҢиҺ«иҝҮдәҺеҝҷзқҖй—№жө·зҡ„е“Әеҗ’дәҶгҖӮдёҖеҸҘвҖңжҲ‘е‘Ҫз”ұжҲ‘дёҚз”ұеӨ©вҖқзҡ„е‘җ
дёҖеҝғдёҖзӣҠпјҢдёҺзҲұеҗҢи·‘пјҢ第еӣӣеұҠе…¬зӣҠи·‘жҠҘ
дҪңиҖ…пјҡpear
иҰҒиҜҙд»Ҡе№ҙи°ҒжңҖеҮәеңҲпјҢиҺ«иҝҮдәҺеҝҷзқҖй—№жө·зҡ„е“Әеҗ’дәҶгҖӮдёҖеҸҘвҖңжҲ‘е‘Ҫз”ұжҲ‘дёҚз”ұеӨ©вҖқзҡ„е‘җ





 жҸҗеҚҮеҚЎ
жҸҗеҚҮеҚЎ зҪ®йЎ¶еҚЎ
зҪ®йЎ¶еҚЎ жІүй»ҳеҚЎ
жІүй»ҳеҚЎ е–§еҡЈеҚЎ
е–§еҡЈеҚЎ еҸҳиүІеҚЎ
еҸҳиүІеҚЎ еҚғж–ӨйЎ¶
еҚғж–ӨйЎ¶ жҳҫиә«еҚЎ
жҳҫиә«еҚЎ ( D1 F: h* t; Y4 e# N+ s V4 C
( D1 F: h* t; Y4 e# N+ s V4 C