本帖最后由 老马 于 2013-2-23 11:27 编辑
MET inhibition in lung cancer
http://www.tlcr.org/article/view/813/1406
Introduction Other SectionIntroduction Met discovery and mechanism of action Met pathway and cross-talks MET and NSCLC Met inhibitors Conclusions AcknowledgementsReferences
The discovery of new cancer-driver genes and the enforcement of molecules targeting them have changed the landscape of Non Small Cell Lung Cancer (NSCLC) treatment.
As a matter of fact, the previous scenario of advanced NSCLC treatment has been completely revolutionized, switching from a “one size fits all” approach to a personalized therapy.
Somatic mutations of the Epidermal Growth Factor Receptor (EGFR) tyrosine kinase domain positively correlated with clinical responsiveness to specific inhibitors: gefitinib, erlotinib and afatinib, two reversible and one irreversible EGFR inhibitors, have consistently demonstrated significant increase of Response Rate (RR) and Progression-Free-Survival (PFS) compared to standard chemotherapy in EGFR mutated NSCLC patients with advanced disease (1-7).
The Anaplastic Lymphoma Kinase (ALK), firstly identified from a chromosomal translocation leading to the production of merged proteins in Non-Hodgkin lymphomas, was then detected as a fusion with the echinoderm microtubule-associated protein-like 4 (EML4) in 6.7% of NSCLC patients (8,9). Crizotinib (PF02341066, Xalkori) targets EML4-ALK thus gaining astonishing response rates in a phase I/II trial and more recently in a phase III trial (10,11).
Unfortunately, other biomarkers already identified in NSCLC are still “undraggable” and one clear example is KRAS. KRAS is a member of the RAS family of oncogenesis, involved in signal transduction and tumorigenesis and its mutations, frequently in codons 12 and 13, have been reported in 20-30% NSCLCS (12-15). Some sign of activity came in the last year from a targeted agent (Selumetinib), which compared to standard chemotherapy in KRAS mutated patients gave interesting results in terms of RR and PFS (16).
Several other molecular markers’ alterations have been described in NSCLC such as: phosphatidylinositol 3-kinases (PI3K) (2%), lipid kinases that regenerate a key mediator between growth-factor receptors and intracellular downstream signaling pathways; ERBB-2 (2%); B-RAF (1-3%), a Ser-Thr kinase that links RAS GTPases to downstream proteins of the MAPK family, thus controlling cell proliferation; ROS1 (about 1%), oncogene that encodes a transmembrane tyrosine kinase receptor; AKT; RET and MET (17-21).
Since the first MET pathway description, several inhibitors have been preclinically and clinically tested, both alone and in combination with chemotherapy or other targeted therapies.
This paper will focus on MET biology, its role in the cell function and tumorigenesis, specifically in lung cancer, as well as on the molecules that target it.
--------------------------------------------------------------------------------
Met discovery and mechanism of action Other SectionIntroduction Met discovery and mechanism of action Met pathway and cross-talks MET and NSCLC Met inhibitors Conclusions AcknowledgementsReferences
Met is a heterodimer receptor tyrosine kinase composed of a α-chain and a β-chain, linked by a disulphide bond.
Met was originally isolated as the product of a human oncogene, trp-met, in tumor cells treated with a chemical carcinogen. Met gene encodes a 170-kD protein (p170met) that has constitutive and ligand-independent tyrosin-kinase activity. Met has pivotal functions in embryogenesis and organogenesis of placenta, liver, kidney, neurons and muscles (22-25).
Moreover, in vivo, Met receptor activation determines a phenomenon called “invasive growth”, which includes cell proliferation, scattering, survival, motility and invasion, epithelial-mesenchymal transition and branched morphogenesis (26,27).
The natural ligand for this receptor is the HGF, produced by stromal and mesenchymal cells, that acts primarily on Met-expressing epithelial cells in an endocrine and/or paracrine fashion (24,28). HGF-induced Met tyrosine kinase activation is regulated by paracrine ligand delivery, ligand activation at the target cell surface and ligand-activated receptor internalization and degradation (29). Going more into details, when HGF binds to the Met receptor, Met major autophosphorylation sites (located within the tyrosine kinase domain) are phosphorylated, with subsequent intrinsic catalytic activation of multiple signaling cascades involved in cell proliferation, survival, angiogenesis, morphogenesis, cell scattering, motility, migration and invasion. An activated docking site in the kinase domain further recruits intracellular adaptor molecules through the SH2 domains and other recognition motifs, such as GAB1 (a key coordinator of the cellular responses to Met). Downstream signaling of the GRB2-mitogen-activated protein kinase (MAPK) cascade, PI3K-mTOR pathway, and STAT pathway are eventually activated, mediating various cellular functions (27,30,31). Finally, in order to activate the receptor, proteolytic cleavage of proHGF is necessary (25).
HGF is mainly produced by stromal tissue like liver and bone marrow, and is expressed in a multitude of mesenchymal-derived cells. Being Met expression detected in the epithelium of most tissues, this indicates that HGF-Met signal transduction pathway contributes to mesenchymal-epithelial interactions (24,32-34).
Met downregulation occurs through rapid internalization of Met itself and subsequent degradation by the lysosome: this process is regulated by ligand-dependent ubiquitination of Met, a process also modulated by specific tyrosine phosphatases and recently identified as proteins decorin and LRIG1 (35,36).
Met can be altered through receptor overexpression, genomic amplification, mutations or alternative splicing. These alterations lead to signaling deregulation that can be mediated through ligand (HGF)-independent receptor activation or through its ligand (HGF)-dependent activation via autocrine (intratumoral HGF), paracrine (mesenchymal or microenvironmental HGF), or endocrine (circulatory HGF) loop signaling cascades (29).
HGF and Met are highly expressed in various stem and progenitors cells, but are only expressed as low levels in their mature cells (25). In preclinical animal models, whereas the overexpression of Met and/or HGF has been shown to stimulate tumorigenesis and metastasis, down-regulation of Met or HGF expression resulted in increased apoptosis and decreased tumor growth and blood vessel density (37-40). Moreover, Met interacts synergistically with VEGF to promote angiogenesis, cell proliferation and invasion (41). This occurs through the transcriptional up-regulation of the hypoxia inducible factor-1α and amplified HGF signaling, that resulted in both induction of invasion and increased expression of VEGF (41).
Met pathway is also one of the key players in the development of acquired resistance to VEGF pathway inhibitors: the inhibition of Met expression prevented hypoxia-induced invasion growth (42,43).
The increased Met expression described in case of response to ionizing radiation through the ATM-NFκB signaling pathway, could lead to radioresistance and cancer invasion (44).
--------------------------------------------------------------------------------
Met pathway and cross-talks Other SectionIntroduction Met discovery and mechanism of action Met pathway and cross-talks MET and NSCLC Met inhibitors Conclusions AcknowledgementsReferences
The cross-talk of Met with various signaling pathways is described in literature and that one between Met and EGFR/HER family receptors is particularly important in lung cancer (45-49).
Met and EGF family receptors are often described co-expressed in tumors and transactivation of Met depends on elevated expression of EGFR in many human tumors (46,50,51). Conversely, HGF stimulation promotes transactivation of EGFR in multiple cell lines, including NSCLC (49).
Cooperation between Met and EGFR occurs also indirectly: when Met activates Src, this lead to EGFR phosphorylation and the creation of docking sites for EGFR interactors involved in downstream signaling (52).
Moreover, through receptor cross-talk, Met exerts a key role in the development of resistance to EGFR family inhibitors. One example is the stimulation of HER-3 phosphorylation and signaling to Akt (a key signaling molecule required for cell survival and proliferation) when Met is amplified and overexpressed (53,54). Inhibition of Met in EGFR inhibitors resistant cells, either in vitro or in vivo, promotes apoptosis, tumor growth reduction and significant necrosis (49,53).
Met and EGFR inhibitors combined together, cooperatively abrogate ErbB3 signaling activation (49). An alternative mechanism in this context is the Src-induced EGFR phosphorylation (52).
Preclinical data also support that Met cross-talks and cooperates with other members of the EGF receptor family, including HER2, to enhance cell invasion and this lead to the possibility to explore therapeutic activity of dual Met and HER2 therapies (55,56).
Stimulation with both HGF and EGF enhances downstream activation of several signaling pathways including Akt, Erk and STAT3 in a way that Met inhibitors abolished their baseline phosphorylation (57,58).
The already mentioned interaction between decorin and LRIG1 proteins, promotes ligand-independent receptor downregulation and degradation of EGFR family members. Decorin binds to the EGFR family, inducing receptor dimerization, internalization and eventual lysosomal degradation, whereas LRIG1 and EGFR associated via their extracellular domains, allow enhanced EGFR phosphorylation. Thus, Met promotes resistance to VEGFR and EGFR inhibitors (59,60).
Cross-talk between Met and KRAS signaling has also been described both in preclinical and clinical findings (61,62). Met activates RAS directly or via a protein-tyrosine phosphatase (63). Similarly, PI3K could be directly activated by Met or indirectly by RAS protein (30).
Moreover, Met directly binds to and sequesters the Fas receptor. This interaction prevents Fas self-aggregation and ligand binding, thus inhibiting Fas activation and apoptosis (64).
Finally, preclinical studies exploring a combination of anti-Met therapeutic agents with mTOR inhibitors have also demonstrated an increased growth suppression, compared to mTOR inhibitors alone (62).
Met plays also a functional role in signaling pathways mediated by other membrane proteins. Integrin-dependent signaling could trigger ligand-independent Met phosphorylation following cellular adhesion, and Met and integrins might have independent yet synergistic roles in cell invasion. Plexins, single-pass transmembrane receptors for semaphorins, acts cooperatively with Met for cell adhesion and migration (45).
--------------------------------------------------------------------------------
MET and NSCLC Other SectionIntroduction Met discovery and mechanism of action Met pathway and cross-talks MET and NSCLC Met inhibitors Conclusions AcknowledgementsReferences
Met receptor is overexpressed in both Small Cell Lung Cancer (SCLC) and NSCLC, mainly in non-squamous histotype (65-67).
Recent tumor microarray expression analysis demonstrated a 72% Met expression in human lung cancer tissue and 40% Met receptor over-expression; such values are higher than in breast (16%) and ovarian cancer (31%), but lower than in renal (70%) and colorectal cancers (CRC; 78%) (67). Phospho-Met expression is found to be at the highest levels in lung cancer (73%), followed by ovarian (33%), breast (23%), and renal (18%) cancer (67).
Met gene amplification can guide the dependency of cell survival and proliferation upon the Met signaling, even in lung cancer cell lines. Blocking Met causes significant growth inhibition, G1-S arrest and apoptosis in cell lines harboring Met gene amplification. When Met is not amplified, its levels of activation are low and cells are unable to grow (68).
Different studies have reported primary Met amplification to be in the wide range of 2% to 21%, in NSCLC lung adenocarcinomas, particularly in TKI-naïve cohorts (69-72).
In lung cancer, Met receptor mutations were mainly found clustered in the non-tyrosine kinase domain, in the juxtamembrane (JM) domain and in the sema domain (67). These mutations are oncogenic activating variants, that result in a deletion in the juxtamembrane domain with enhanced oncogenic signaling, tumorigenicity, cell motility, and migration (27,73). Met kinase domain mutations have been found to be somatically selected in the metastatic tissues, compared with the primary solid cancers (74).
Literature data are quite discordant on the prognostic value of Met over-expression, amplification and mutation.
The overexpression of circulating Met in patients with NSCLC has been strongly associated with early tumor recurrence and patients with adenocarcinoma and Met amplification have also demonstrated a trend for poor prognosis (69,75,76).
Concerning the correlation between Met FISH status and clinical characteristics, only Okuda and colleagues demonstrated an association with male gender and smoking status, showing also a relationship with high Met gene copy number (77). In the same trial, both FISH positive and gene amplified cases had a worse prognosis, although the difference was not statistically significant and among the Met FISH-positive NSCLCs, patients with gene amplification showed not significantly worse OS compared to those with high polysomy.
All FISH-positive cases had squamous histology, adenocarcinoma had Met amplification: high Met gene copy number tended to have shorter OS and PFS than those with low Met gene copy number, being this difference statistically significant only in the squamous histotype.
Moreover, at multivariate analysis done on squamous histology, increased Met gene copy number and Met amplification were confirmed to be independent poor prognostic factors.
No significant difference in prognosis was found in patients having adenocarcinoma regardless Met FISH status in the korean study. In contrast, Beau-Faller and colleagues found a tendency toward shorter event-free survival in adenocarcinoma patients with increased Met gene copy number, whereas Kanteti and colleagues demonstrated that the high Met gene copy number in adenocarcinoma was associated with a trend of better prognosis (69). However, the above mentioned study has some critical methodology aspects as it was conducted on a small sample size and qPCR was used as test and not FISH, done on DNA samples extracted from formalin-fixed paraffin-embedded (FFPE) archival tumor tissues (70).
Capuzzo and colleagues found no patient with EGFR mutation was Met FISH positive, but increased Met gene copy number significantly correlated with EGFR FISH-positive status (78).
Acquired Met amplification has also been linked to approximately 22% of non-T790M mediated secondary gefitinib resistance in NSCLC patients, although it can also occur concurrently but independently (52,53,78-80).
Using in vitro cell line models, the Met gene amplification in gefitinib-resistant cell clones was identified (53).
Rho and colleagues tried to demonstrate that Met activation, rather than gene amplification, is sufficient to promote EGFR resistance, but the activation appear to be secondary to increase passage numbers rather than to EGFR-Tki exposure (81).
More recently, two prospective analyses have investigated the mechanism of EGFR-Tki resistance through the tissue rebiopsy: high Met gene copy number was found in 11% and 5% of the tissue samples, respectively (82,83).
--------------------------------------------------------------------------------
Met inhibitors Other SectionIntroduction Met discovery and mechanism of action Met pathway and cross-talks MET and NSCLC Met inhibitors Conclusions AcknowledgementsReferences
Several inhibitors have been tested so far: they can be classified according to their mechanism of action in selective Met inhibitors, unselective Met inhibitors and antibodies targeting Met or HGF (Figure 1, Table 1).
Table 1 Ongoing trials on Met inhibitors
Full table Figure 1. Met inhibitors in the clinic Selective Met inhibitors
Tivantinib
Tivantinib (ARQ 197) is the first non-ATP-competitive small molecule that selectively targets the Met RTK, locking and stabilizing the kinase in a “closed” and “inactive” conformation, causing the disruption of Met phosphorylation and the downstream signaling.
Moreover, tivantinib enhances Met degradation through the ubiquitin/proteasome pathway in vitro, induces apoptosis in Met activated cell-lines and it’s active in multiple human cancer xenografts (84,85).
Tivantinib acts synergically with antiangiogenentc drugs in preclinical studies on solid tumor cell lines (86).
Studies in vitro and in vivo demonstrated its activity in several types of cancer such as breast, colorectal and gastric cancer (85,87).
Met cancer expressing cell lines treated with tivantinib displayed either a dose-dependent loss of proliferative capacity or caspase-dependent Met apoptosis, which positively correlated with either ligand-dependent Met activity or constitutively active Met. Tivantinib does not exert any activity in cancer cell lines not expressing Met or phospho-Met.
Tivantinib has been investigated in three phase I trials, as single agent and in combination.
In the first dose-escalation phase I trial, tivantinib is administered as single-agent in patients with advanced solid tumors. Initially, an intermittent dosing was planned but, due to the bradycardia experienced in the other phase I trial using this schedule, the protocol was amended and the following 79 patients received a continuous dose (88).
No MTD was reached in this study and less than 33% of patients experienced DLTs at any given dose. Thus, the recommended phase II dose was confirmed at 360 mg twice a day as per a concomitant phase I study, where this MTD was identified (88).
The most commonly reported drug-related adverse events of any grade included fatigue, gastrointestinal (GI) disorders (nausea, vomiting and diarrhea) and anemia.
Pharmacokinetic was linear. There was considerable inter-patient variability, but no relationship between drug-related adverse events (AEs), dose and extent of tivantinib exposure; consequently, this inter-patient variability was not considered relevant for its clinical safety. Partial responses registered in this trial were equal to 4.8% (89).
In another phase I trial, two formulations of tivantinib were tested: the amorphous and the crystalline A formulation. The trial was lead in a single institution, the Royal Marsden Hospital (Sutton, United Kingdom) and highlighted the following DLTs: one patient had grade 3 fatigue at 200 mg, one patient presented a grade 3 febrile neutropenia, one other a grade 3 mucositis, one a grade 3 palmar-plantar erythrodysesthesia and one a grade 3 hypokalemia at 400 mg. The MTDs- recommended phase 2 doses (RP2Ds) were 300 mg bi-daily for the amorphous formulation and 360 mg bi-daily for the crystalline A formulation. The main grade 1-2 AEs, all generally self-limiting, were fatigue (15.7%), nausea (13.7%), vomiting (11.8%). Tivantinib is metabolized by CYP2C19: one patient with CYP2C19 deficiency experienced grade 4 febrile neutropenia and grade 3 mucositis as the drug’s AUC was 3-fold higher (90).
The crystalline A formulation of tivantinib resulted in lower drug exposure at 300 and 360 mg twice daily, compared with the amorphous form at 300 mg twice daily (likely due to different dissolution characteristics). RECIST stable disease ≥4 months was the best response in 14 patients, together with minor tumor regressions (88).
As the ratio of the poor metabolizers of CYP2C19 in Asians is around 20% (while is very low in Caucasians), a Japanese phase I trial was designed to evaluate drug’s safety profile of tivantinib in this group of patients with metastatic solid tumors and the drug was well tolerated, but CYP2C19 genotype clearly affected the exposure and the RP2Ds differed for “no poor metabolizers” (360 mg bi-daily) and for “poor metabolizers” (240 mg bi-daily). Most common AEs were similar to those mentioned above (91). A phase III trial was conducted in Asia in advanced NSCLC patients, comparing erlotinib + tivantinib versus erlotinib + placebo at the dose calculated considering the CYP2C19 polymorphism (92). A press release in August 2012 announced a suspension in the accrual for this study, due to suspected cases of interstitial lung disease (93).
Based on the preclinical data showing a synergistic action between EGFR-TKi and Met inhibitors, an open-label sequential dose escalation phase I trial on tivantinib + erlotinib was set up. Thirty-two metastatic cancer patients were included: 59% were males, 75% PS 1 and mean age was 60 years. The MTD was not established, however, the RP2D was 360 mg bi-daily for tivantinib and 150 mg daily for erlotinib. Two DLT were experienced at 360 mg (grade 4 neutropenia, grade 3 thrombocytopenia), none at 240 or 120 mg. The most common AEs were cutaneous rash, fatigue, nausea, abdominal pain, diarrhea, bradycardia and anemia, mostly grade 1 and 2. No drug related death, but 11% grade 3-4 neutropenia and 8% grade 3-4 nausea were recorded (94).
This combination of erlotinib (150 mg daily) + tivantinib (360 mg bi-daily) every 4 weeks was further studied in a phase II, double-blind, randomized open-label study in comparison with erlotinib 150 mg daily + placebo, in previously treated locally advanced or metastatic NSCLC patients. One hundred and sixty-seven patients were enrolled and homogeneously distributed between the two arms (mainly males, never or former smoker, with stage IV disease and adenocarcinoma histology): 10% in the combination arm versus 18% in the standard arm presented an EGFR mutation, 10% versus 17% a KRAS mutation, 26% versus 26.5% had 4 or more MET gene copy number. The ORR was 10% for erlotinib + tivantinib versus 7% for the control arm.
Median investigator’s PFS was 3.8 months for the tivantinib + erlotinib arm versus 2.3 months for the erlotinib + placebo arm (HR=0.81, P=0.24); the reviewer’s PFS was 3.6 versus 2 months (HR=0.74, P=0.09). Median OS was 8.5 for the investigational arm versus 6.9 months for the control arm (HR=0.87, P=0.47). Pre-planned exploratory survival analysis in non-squamous histology showed a trend of benefit from the combination arm in both PFS (HR=0.71) and OS (HR=0.72). Even in a small number of patients, the subgroup analysis showed an advantage in terms of PFS for EGFR wild type (HR=0.70), KRAS mutated patients (HR=0.76) and for Met FISH positive patients (>5, HR=0.45).
Treatment was well tolerated both in the investigational and in the control arm: low grade rash (9.5% versus 7.2%) and diarrhea (7.1% versus 7.2%), fatigue (4.8% versus 6%), nausea (1.2% versus 4.8%), vomiting (3.6% versus 1.2%), dyspnea (7.1% versus 13.3%), anemia (6% versus 7.2%) were the most common reported toxicities (95).
On the basis of data coming from this phase II trial, the phase III MARQUEE trial was designed in non-squamous NSCLC patients with the same schema, having the overall survival (OS) as primary end-point. Unfortunately, a press release in October 2012, revealed that the primary end point in the intent to treat population was not met, but no further data are yet available (96,97).
Others selective Met inhibitors
PF-04217903 is a selective ATP-competitive small inhibitor of Met kinase. It inhibits tumor cell proliferation, survival, migration/invasion in Met-amplified cell lines in vitro, and shows marked antitumor activity in tumor models harbouring either Met gene amplification or a HGF/Met autocrine loop. PF-04217903 also demonstrates potent antiangiogenic properties in vitro and in vivo (98). In 2012 a phase I trial with PF-04217903 in patients with advanced solid tumors was prematurely discontinued, due to strategic development decision by Pfizer. No safety concerns were reported (99).
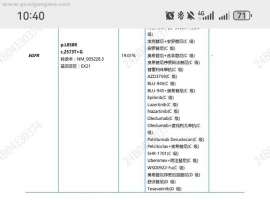
AMG 337 is a selective inhibitor of the proto-oncogene Met thereby disrupting Met signal transduction pathway. A phase I, open-label, sequential dose escalation and expansion study with AMG 337 in subjects with advanced solid tumors is currently ongoing (100) (Table 1).
INCB028060 is an oral potent and highly selective Met inhibitor, capable of suppressing tumor growth in vivo at doses that are extremely well tolerated (101,102).
Good tolerance was confirmed in a phase I standard 3+3 dose-escalation study once or twice daily on a continuous 28-day schedule in patients with advanced solid tumors. The MTD was not reached and no grade 3-4 AEs were noted, except grade 3 ALT increase in a patient with liver metastases and grade 2 ALT levels at baseline. Grade 1-2 AEs experienced were mild tremor, fatigue, nausea, diarrhea, indigestion and headache (103).
Non-selective Met inhibitors
Crizotinib
Crizotinib was synthesized primarily as a Met inhibitor. It was engineered based on interactions of a precursor (PHA-665752) with the ATP-binding sites of the Met kinase domain thus resulting in displacement of the kinase activation loop, that interferes with ATP and substrate binding to the Met receptor tyrosine kinase. Crizotinib was designed in order to be less lipophilic and to have a small hinge binder with the possibility to better interact in the kinase pocket (104).
Crizotinib was proved to be active in NSCLC cell lines carrying Met amplification. However, no activity was described in Met mutated, EGFR mutated or normal cell lines. Moreover, crizotinib markedly inhibited AKT, Met and ERK phosphorylation. By doing that, it induced apoptosis even though a mediation of BIM up-regulation (pro-apoptotic member of the Bcl-2 family) and survivin down-regulation (a member of the inhibitor of apoptosis protein family) has also been reported.
Interestingly, in Met or EGFR mutated but also in normal cell lines, whit a low Met phosphorylation, the Met phosphorylation is completely inhibited, whereas the ERK and AKT are not (105).
During drug development, Ou and colleagues described a case of prolonged partial response to crizotinib in a NSCLC patient carrying Met amplification (defined as Met/CEP7 ratio >5) but no ALK translocation (106).
The first phase I trial was designed as open-label, multicenter, to evaluate safety and efficacy of crizotinib: this study was emended with an expanded cohort for patients with lung cancers carrying ALK rearrangements. The recommended crizotinib dose was 250 mg twice daily in 28-day cycles.
In the overall NSCLC population a phase I trial investigated crizotinib in association to dose escalating erlotinib: 5 DLTs were reported (at 150/100 mg grade 2 vomiting, grade 2 esophagitis and dysphagia, grade 3 diarrhea and dehydration; at 200/100 mg, grade 3 dry eye and grade 3 esophagitis). Ninety-two percent of the patients experienced treatment-related AEs, mainly grade 1 or grade 2: diarrhea (72%), rash (56%) and fatigue (44%) (107).
Another phase I trials evaluated crizotinib in combination with dacomitinib, an irreversible pan-erb inhibitor in previously treated advanced NSCLC patients (108).
Cabozantinib
Cabozantinib (XL184) is a potent Met/VEGFR2/RET/KIT/AXL/FLT3 inhibitor that targets tumor survival, metastasization and angiogenesis.
It selectively inhibits KIT, RET, AXL, TIE2 and FLT3 (all kinases implicated in tumor pathobiology) through strong, reversible, ATP-competitive binding. Moreover, cabozantinib inhibits HGF and VEGF-mediated cell migration and also Met and VEGFR phosphorylation and the tubule formation, with no evidence of cytotoxicity.
This effect described in vitro, turned into in vivo significant tumor regression, without any relevant toxicity (109).
Several phase I trials have already been published verifying the schedule, the formulation, the dose of the drug, both as single-agent and in combination with other molecules.
Kurzrock and colleagues studied single-agent cabozantinib both in suspension and capsule formulation, at intermittent (5 days on, 9 off) and continuous schedule: MTD was defined at 175 mg continuous schedule, being DLT mucositis, elevated lipase and altered liver function (110).
The continuous dose was further investigated in a Japanese only population: MTD was 60 mg, being grade 3 hypertension the DLT (111).
Regarding combination regimens, a phase I study analyzed the interaction of the combination cabozantinib and rosiglitazone, as the latter is a CYP2C8 substrate, but no interaction was found between these two compounds (112,113).
Cabozantinib was further studied in several phase II trials in different tumor types. Among them, one phase II trial investigated treatment with cabozantinib in NSCLC patients previously treated with anti-EGFR TKi (50%) and anti-VEGF therapies (32%). At week 12 the ORR was 10% and the overall DCR 40%. No difference in terms of PFS (median 4.2 months) was seen in the two populations according to the treatment response at 12 weeks. The most common grade 3-4 events were diarrhea (7%), palmar-plantar erythrodyesthesia (8%), fatigue (13%) and asthenia (7%) (114).
Likewise tivantinib, also cabozantinib was tested together with erlotinib or gefitinib in vivo and in vitro in EGFR TKi resistant NSCLC xenograft models harboring Met amplification. Gefitinib and cabozantinib were tested on gefitinib resistant cell lines either alone and in combination and the two molecules together were substantially more potent than each drug alone (>50% inhibition). The same result was obtained with the combination of erlotinib and cabozantinib on erlotinib resistant cell lines (115).
The combination of cabozantinib and erlotinib was tested on 54 NSCLC patients in a phase Ib/II study. Patients were divided into 5 cohorts in two parallel arms: arm A (75 mg cabozantinib + 100 mg erlotinib; 125 mg cabozantinib + 100 mg erlotinib; 125 mg cabozantinib + 50 mg erlotinib) and arm B (75 mg cabozantinib +150 mg erlotinib; 50 mg cabozantinib +150 mg erlotinib). Twelve patients experienced at least 1 DLT: diarrhea, increased AST levels, palmar-plantar erythrodysesthesia, mucositis, hypertension, hypokalemia, elevated lipase and fatigue. The most common grade 3-4 adverse events were diarrhea (26%), fatigue (15%), dyspnea (12%) and hypoxia (9%) (116).
In advanced NSCLC patients two phase II trials are ongoing: the first one randomizes EGFR wild type patients to erlotinib, cabozantinib or erlotinib plus cabozantinib as second or third line therapy; the second study investigates cabozantinib in patients with KIF5B/RET positive NSCLC (117,118) (Table 1).
Foretinib
Foretinib (XL-880, EXEL-2880) is an oral multi-kinase inhibitor developed to target Met and several other receptor tyrosine kinases involved in tumor angiogenesis. It is an ATP-competitive inhibitor and binds the ATP pocket of both Met and VEGFR-2 tyrosine kinase domains with high affinity.
Both in vitro and in vivo, foretinib inhibits Met and VEGF receptor-2 (VEGFR-2) and have high in vitro affinity for PDGFRb, Tie-2, RON, Kit, and FLT3 kinases, preventing tumor growth through a direct effect on tumor cell proliferation and inhibition of invasion and angiogenesis, mediated by HGF and VEGF receptor (119).
Two phase I trials have been published: the first investigated foretinib administered for 5 consecutive days every 14 days in a 3+3 dose escalation study; in the second study foretinib was administered once daily for 28 days. Both trials were conducted in patients with metastatic or unresectable solid tumors. MDT was defined as 3.6 mg/kg for 5 consecutive days every 14 days in the first study and as 80 mg daily in the second; DLTs in the first study included grade 3 elevations in aspartate aminotransferase and lipase, whereas in the second trial hypertension, dehydration and diarrhea were described.
Additional AEs in both studies included hypertension, fatigue, diarrhea, vomiting, proteinuria, and hematuria. In these studies no responses were observed and most of patients achieved a stable disease as best response (120,121).
A phase I, open-label, randomized, 2-part crossover study assessed the safety, pharmacokinetics and relative bioavailability of single doses of foretinib free base tablet formulation compared to a bisphosphate salt capsule formulation: both were well tolerated and their pharmacokinetics and relative bioavailability were not clinically different (122).
On the basis of preclinical data, showing that combining foretinib with erlotinib or lapatinib effectively decrease the phosphorylation of Met, HER1, HER2, HER3, AKT, and ERK in cell lines, a phase I/II study of erlotinib in association or not with foretinib in previously treated NSCLC patients has been designed and is currently ongoing (123,124) (Table 1).
Golvatinib
Golvatinib (E7050) is a novel small molecule ATP-competitive inhibitor of Met receptor, that potently and selectively inhibits the autophosphorylation of Met and VEGF-induced phosphorylation of VEGFR (125).
Golvatinib also circumvents resistance to reversible, irreversible, and mutant-selective EGFR-TKIs induced by exogenous and/or endogenous HGF in EGFR mutant lung cancer cell lines, by blocking the Met/Gab1/PI3K/Akt pathway in vitro and also prevents the emergence of gefitinib-resistant cells, induced by continuous exposure to HGF (126).
A phase I study with oral daily golvatinib administered continuously once a day in patients with advanced solid tumors was performed. Three DLTs were observed: grade 3 increase in GGT and alkaline phosphatase levels and grade 3 fatigue, all at 450 mg. The MTD was determined to be 400 mg every day. Frequently occurring AEs were fatigue (68%), diarrhea (65%), nausea (62%), vomiting (53%), decreased appetite (47%), ALT increase (38%) and AST increase (23%). No grade 4 AEs were observed (127).
Other molecules
MGC D265 is an oral receptor tyrosine kinase inhibitor targeting Met, VEGF, RON and Tie2. Preclinical data have demonstrated synergism of action with erlotinib and early clinical trials are currently ongoing (128) (Table 1).
ANG707 is another non-selective Met inhibitor under investigation in early phase trials (129).
Antibodies
Antibodies against Met
Onartuzumab (MetMab)
MetMAb is a recombinant, fully humanized, monovalent monoclonal anti-Met antibody based on the human IgG1k framework sequence. It binds in the sema domain of Met within the extracellular domain, where it acts to inhibit HGF binding and initiation of receptor activation. The unique monovalent design of MetMAb eliminates the potential for Met activation via antibody-driven receptor dimerization (130).
The activity shown in vitro by MetMAb did not translate into a full activity in vivo: only about 65% tumor inhibition was demonstrated, indicating that blockade of HGF by MetMAb is not sufficient for full tumor inhibition in specific tumors (130).
A phase I trial investigated sequential 3+3 dose-escalation of endovenous MetMAb in advanced solid tumors: MetMAb was three weekly intravenously administered, both as single agent and in combination with bevacizumab 15 mg/kg every three weeks, until progression.
Most frequent MetMAb AEs as single-agent were: fatigue (56%), peripheral edema (35%), decreased appetite (32%), constipation (29%), nausea (27%), vomiting (24%) and hypoalbuminemia (24%); there was no consistent relationship between AEs and dose level.
Grade 3 AEs were peripheral edema (9%), abdominal pain, AST increase, fever and hyponatremia. No Grade 4 toxicity was observed. The combination arm had similar toxicities; no grade 3 or 4 toxicity was experienced. MTD was not reached. The best response was stable disease (131).
The phase II trial was a global, randomized, double-blind trial evaluating the combination of MetMAb + erlotinib versus placebo + erlotinib in second/third line NSCLC advanced patients. One hundred and twenty-eight NSCLC patients were enrolled with a baseline immunohistochemical evaluation of Met: 54% of the patients were considered as Met positive (high protein expression at IHC). Met positive patients treated in the experimental arm had a significantly higher PFS (3.0 vs. 1.5 months; HR 0.47; P=0.01) and OS (12.6 vs. 4.6 months; HR 0.37; P=0.002) (132).
Based on phase II data, a randomized, phase III, multicenter, double-blind, placebo-controlled study evaluating the efficacy and safety of onartuzumab in combination with erlotinib in patients with Met positive NSCLC who have received standard chemotherapy for advanced disease is currently recruiting patients (133) (Table 1).
The positive results of the phase I trial on MetMAb in combination with bevacizumab have paved the way to the ongoing randomized phase II multicentric double-blind placebo-controlled study evaluating the efficacy and safety of MetMAb in combination with either bevacizumab + platinum + paclitaxel or pemetrexed + platinum as first-line treatment in patients with stage IIIB and IV non-squamous NSCLC (134).
Antibodies against HGF
Ficlatuzumab
Ficlatuzumab (AV-299) is a potent hepatocyte growth factor (HGF) inhibitor IgG1 monoclonal antibody, that binds to the HGF ligand with high affinity and specificity. Ficlatuzumab was studied in two phase I trials and one phase II study. In both phase I trials it was associated with gefitinib and erlotinib. In the first phase I trial ficlatuzumab was biweekly administered intravenously over 30-60 minutes both as single-agent and in combination with erlotinib at 150 mg continuously in advanced solid tumors. There were no DLT in the monotherapy arm; consequently no MTD was identified.
For the combination arm there was one DLT (grade 3 mucositis). The RP2D for both monotherapy and combination regimen was defined as 20 mg/kg every 2 weeks. Ficlatuzumab as a single-agent demonstrated a stabilisation of disease in 50% of the cases (135).
The second phase Ib trial enrolled only Asiatic patients with unresectable NSCLC: ficlatuzumab was administered intravenously every 2 weeks at two dose levels (10 and 20 mg/kg) in combination with gefitinib at 250 mg daily. No DLTs were observed in the dose-escalation cohorts; 20 mg/kg of ficlatuzumab every 2 weeks + gefitinib 250 mg daily was selected as RP2D. Among 12 patients in the 20 mg/kg cohort, 5 partial responses were achieved (136). Most frequent treatment-emergent adverse events (AEs) were fatigue (27-33%), dermatitis acneiform (53%, particularly for the combination regimens), diarrhea (33-46%) and edema (16-27%) for both single-agent and combination therapy (135,136).
The efficacy of ficlatuzumab together with gefitinib was further investigated in a multicenter, open-label, exploratory, 2-arm randomized phase 2 study in previously untreated Asian NSCLC patients with the doses defined in the phase I. One-hundred eighty-eight patients were randomized with a baseline evaluation of Met by IHC and gene copy number. In the low Met group, ORR (41 versus 22%) and median PFS (7.3 versus 2.8 m) favored the combination regimen with a manageable toxicity profile (137).
Rilotumumab
Rilotumumab (AMG 102) is a fully human monoclonal antibody that selectively targets and neutralizes hepatocyte growth factor/scatter factor (HGF/SF). It preferentially bound to the β-chain of the human, mature, active form of HGF, and had no apparent effect on proteolytic processing of the inactive HGF precursor (138).
Two phase I trials have been published so far with AMG 102 in advanced refractory solid tumors: one as single agent and one in combination with bevacizumab or motesanib (139).
In the monotherapy trial, AMG 102 was well tolerated up to the planned maximum dose of 20 mg/kg, MTD was not reached and pharmacokinetic was linear. Two patients experienced DLTs: one grade 3 hypoxia and grade 3 dyspnea (0.5 mg/kg cohort) and one grade 3 upper GI hemorrhage (1 mg/kg cohort). Treatment-related AEs were generally mild and included fatigue (13%), constipation (8%), nausea (8%), vomiting (5%), anorexia (5%), myalgia (5%), and hypertension (5%). Seventy percent of the evaluable patients had a SD as best response (139).
The phase Ib combination study sequentially enrolled patients into four cohorts, but the number of those receiving AMG 102 plus motesanib was insufficient to adequately assess safety and the accrual was early suspended because of reports of cholecystitis in other motesanib studies. No dose-limiting toxicities were reported and the combination of AMG 102 with bevacizumab seemed to have acceptable toxicity. AEs were generally mild and included fatigue (75%), nausea (58%), constipation (42%) and peripheral edema (42%) (140).
TAK 701
TAK-701 is a humanized monoclonal antibody that binds HGF thus inhibiting its bound to Met receptor. TAK-701 in combination with gefitinib blocks the phosphorylation of Met, EGFR, extracellular signal-regulated kinase, and AKT in HGF expressing human NSCLC cell lines with an activating EGFR mutation. Combination therapy also markedly inhibited the tumor growth in vivo (141).
Preliminary data of a phase I study in advanced solid malignancies with TAK-701 showed that the most common AEs were cough, abdominal pain, constipation and fatigue, all grade 1-2. There were 3 grade 3 AEs (gastrointestinal ileus, pleural effusion, urinary tract infection) and 1 grade 4 AE (dyspnea). No DLT was found and the MTD has not been reached (142).
--------------------------------------------------------------------------------
Conclusions Other SectionIntroduction Met discovery and mechanism of action Met pathway and cross-talks MET and NSCLC Met inhibitors Conclusions AcknowledgementsReferences
In patients with advanced NSCLC, a correct definition of the histotype is still the first step to design a proper therapeutic algorithm, but personalized molecular diagnosis is becoming more and more relevant.
Genetically defined subsets of cancers may share dependence on a specific signaling pathway: specific inhibitors targeting these pathways would be most effectively tested in patient populations characterized by molecular markers.
Moreover, genetic events that arise and are selected during tumor progression may become essential for tumor survival, a phenomenon generally described as “oncogene addiction”: cancer cells appear to depend on a single overactive oncogene to proliferate and survive (143). Optimal case selection, diagnostic and pharmacodynamic biomarker development, the identification and testing of rationally designed anticancer drugs and combination strategies are crucial to develop the best treatment for the right patient (144).
New generations of molecularly targeted drugs will allow more personalized medicine and more efficacious and less toxic antitumor therapies in patients with defined molecular aberrations, sparing normal cells thus sparing toxicity (145,146).
Met can act as an ‘oncogene expedient’ even in absence of genetic alterations and might potentiate the effect of other oncogenes, promote malignant progression and participate in tumor angiogenesis (147).
Met dysregulation correlates with disease prognosis in numerous cancers and represents a possible target for personalized treatment. The clinical efficacy of Met targeting agents in lung cancer needs further details from the ongoing trials as well as more information are necessary to establish the most appropriate diagnostic test to identify Met expression or amplification.
Several molecules are currently under investigation and two of them already reached phase III trials in advanced NSCLC.
|














 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡